Goals of Patient Care and Residential Goals of Care
- In WA, Goals of Patient Care and Residential Goals of Care are clinical care planning processes completed by your healthcare team in hospitals and residential aged care facilities.
- It helps to plan treatments that would be useful for you if you became unwell and were not expected to get better.
- Goals of care processes use a shared decision-making approach between you and your healthcare team. You may also want to include your family, carers and / or your recognised decision-makers in the conversations.
- If you already have completed an advance care planning document, such as an Advance Health Directive or a Values and Preferences Form your healthcare team will use it as part of the goals of care discussion.
- Together, you decide which treatments would be appropriate and acceptable to you particularly in relation to end of life or terminal care.
Goals of care decisions are made thinking about your current health, your individual healthcare needs, and your preferences for future care. You may also want to describe treatments that you would prefer not to have, as sometimes there are treatments that may cause unnecessary pain or discomfort. If you live in a residential aged care facility you may also want to talk about where you want to be cared for and whether or not you want to go to a hospital for more treatment. You will also be able to ask questions and hear the opinion of your healthcare team about your future care and treatment options.
Talking openly about your goals of care will enable your preferences for care to be discussed and your views to be heard. These discussions should happen regularly with your healthcare team.
Goals of care clinical forms
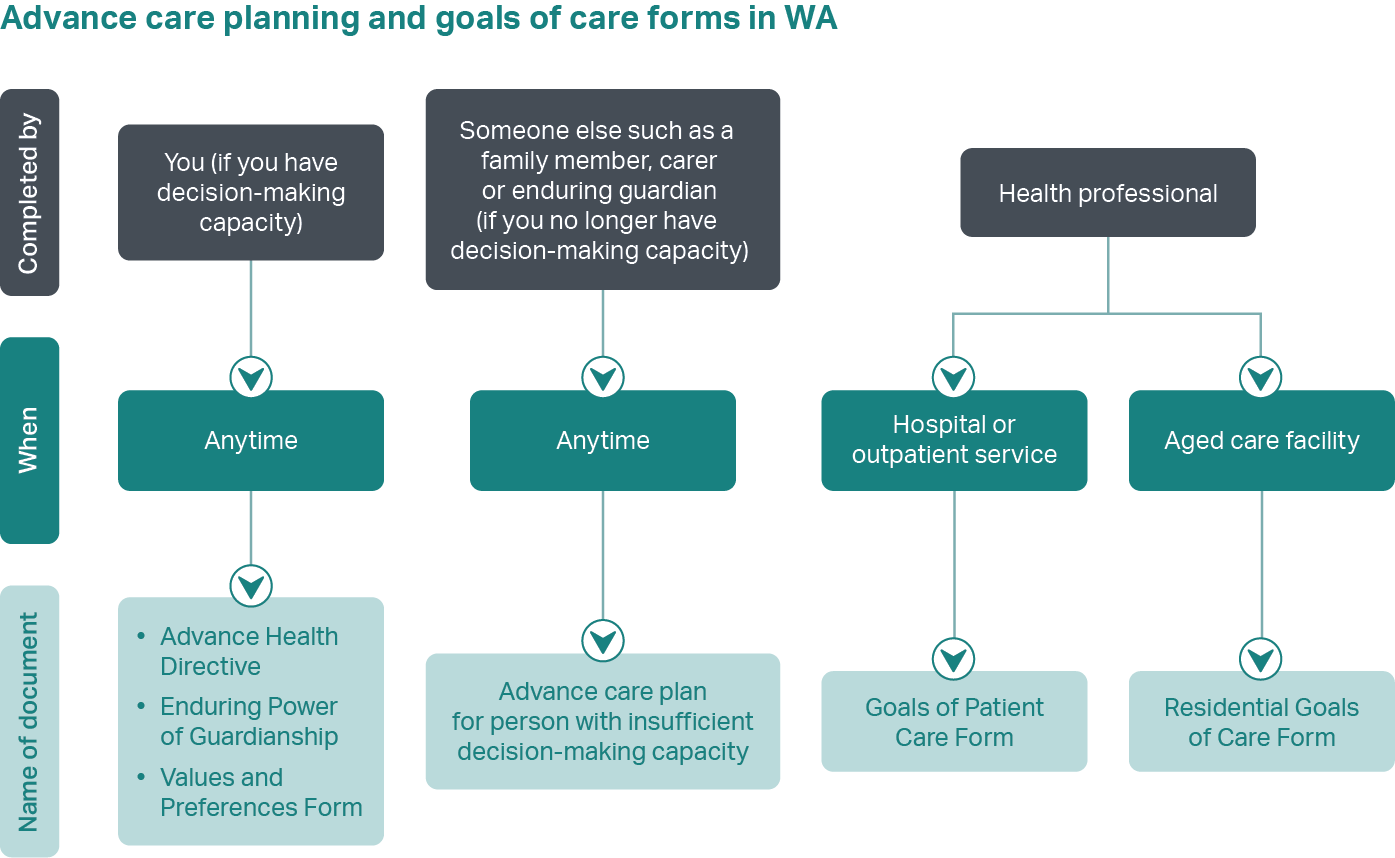
In WA, there are two common goals of care clinical forms written by your healthcare team during goals of care discussions:
- In hospital or at an outpatient appointment – Goals of Patient Care
- In residential aged care facility – Residential Goals of Care
If you are in hospital or at an outpatient appointment, your hospital doctor or medical team will usually lead the conversation. If you are in a residential aged care facility, your treating doctor or a senior health professional will usually lead the conversation.
Talking about your goals of care
When you talk about your goals of care with your healthcare team, you should talk about your current health, your values and preferences for future care. You can also talk about any cultural, spiritual or religious values that you feel are important to your treatment choices and end of life care. The healthcare team will give advice about your health or illness and talk through options for treatments that might be helpful or unhelpful for you.
Goals of care discussions can help plan the type of treatment you would want if your condition gets worse. This might include emergency or life sustaining medical treatments that you may need, for example, cardiopulmonary resuscitation (CPR) or admission to an Intensive Care Unit (ICU). These treatments may impact on your quality of life.
If you are no longer able to make decisions in relation to your goals of care or take part in the discussions, the doctor or healthcare team will involve your recognised decision-maker(s) in line with the Hierarchy of treatment decision makers (external site).
Tips for your goals of care discussions
- Think about what is important to you or what matters the most to you. What is important about your daily life? For your care? What situations or circumstances do you want to avoid?
- Think about your goals for your health care. What is your medical condition? How are you feeling now? How might it change over time? What services and treatments might help you, which ones would you not want?
- Ask your family, carers and/or recognised decision-makers to be there with you for the conversation. It can help them to understand what is important to you. It may also be helpful for them if they are supporting decision-making for you in the future.
- Bring your Advance Health Directive or other advance care planning documents with you if you have one.
Documenting your goals of care
There are lots of treatment options that are recorded by your doctor or healthcare team on the goals of care forms. These only apply if your condition gets worse and you are not expected to get better.
- All life sustaining treatment
All hospital treatments including care within an ICU will be considered. If you are at a residential aged care facility, this will include transfer to hospital for treatment.
- Life extended intensive treatment – with treatment ceiling
Care within a hospital ICU will be considered but not all treatments will be used e.g. you may not wish to have blood products.
- Active ward-based treatment – with symptoms and comfort care
Treatment will be given within a hospital ward but care will not be transferred to an ICU. There will be an emphasis on quality of life and on treatments that will improve comfort but may also extend life.
- Optimal comfort treatment – including care of the dying person
The aim of all treatment will be to provide comfort and prevent and relieve suffering. If you live in a residential aged care facility this treatment is usually provided in the facility by your usual healthcare team. Treatment in hospital is usually only needed if you cannot be kept comfortable in the facility.
When the goals of care form is complete, it is kept in your healthcare notes or file, so other healthcare staff know what you have decided. A copy may be uploaded to the service’s electronic health record if one is available. You may also be asked if you are happy for it to be uploaded to your My Health Record (see section below called 'Goals of Care and My Health Record’). The forms can apply when you are being transferred between different hospitals and facilities.
You can ask to see or discuss the forms at any time.
Changing your mind and updating the form
Your goals of care are likely to change over time, especially as your health changes. You and your family, carer and/or recognised decision maker representative can ask to talk about your goals of care forms at any time. The form can be changed and updated as your health changes.
In residential aged care facilities, the form should be reviewed at least every 12 months.
Goals of care and advance care planning documents
It is a good idea to think about your values and preferences for your future care when you are feeling well and able to make decisions. In WA there are different documents you can use to write down and share these decisions, known as advance care planning documents (e.g.. Advance Health Directive or a Values and Preferences Form). These are completed by you.
If you already have an advance care planning document when you go to hospital, tell your healthcare team and make sure they have a copy in your health records.
A goals of care form is completed by your healthcare team and still useful if you have an advance care planning document. The goals of care form and your advance care planning documents should complement or ‘match’ each other. The goals of care discussion will give you and your healthcare team the chance to:
- check that what is written in your advance care planning document is still up to date
- discuss any other relevant care or treatment options that are not covered by your advance care planning document
- have confidence that the clinician understands your preferences and trust that the treatment you will receive will be consistent with those preferences.
Goals of Patient Care and My Health Record
If you have a My Health Record (MHR), there are some WA Health hospitals that can upload your Goals of Patient Care forms to your record. This can only happen if you agree to this with the doctor at the time of completing the Goals of Patient Care form. Having copies of your Goals of Patient Care form in MHR, allows it to be seen by healthcare professionals involved in your care and can inform ongoing discussions with you about future treatment and care.
If you get admitted to a different hospital, your new healthcare team may review your Goals of Patient Care form in MHR and use it to talk about your goals of care in your new admission.
Like many documents in MHR, you can remove a goals of care form from your record at any time. For further information on how to do this visit My Health Record (external site)
You can also find more information about advance care planning on My Health Record (external site)
Last reviewed: 03-07-2024
Acknowledgements
End-of-Life-Care Program
WA Country Health Service
This publication is provided for education and information purposes only. It is not a substitute for professional medical care. Information about a therapy, service, product or treatment does not imply endorsement and is not intended to replace advice from your healthcare professional. Readers should note that over time currency and completeness of the information may change. All users should seek advice from a qualified healthcare professional for a diagnosis and answers to their medical questions.